
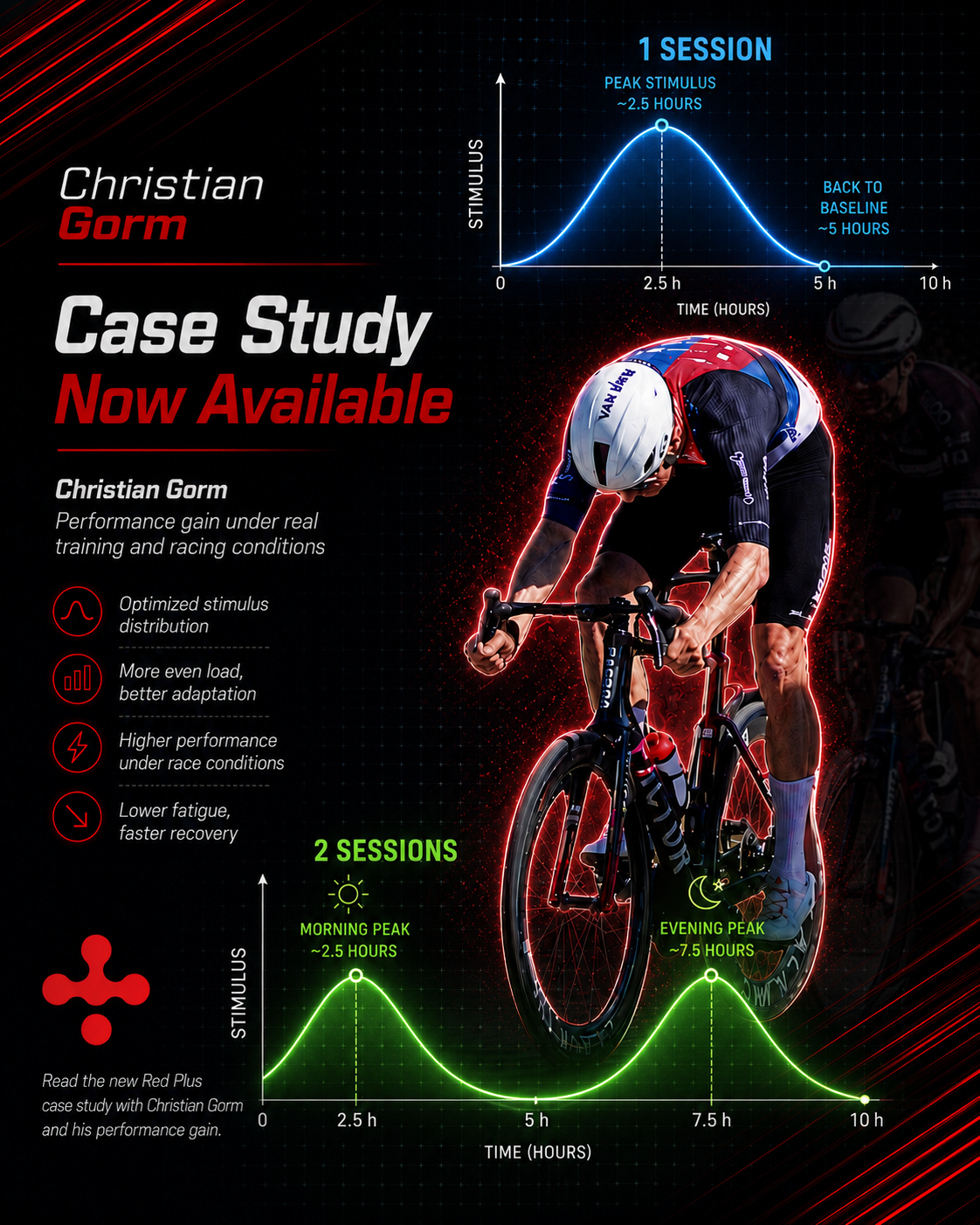
Christian Gorm – RedPlus Beta Tester Case
When peak load, protocol deviation and de acclimatisation reveal a physiological response
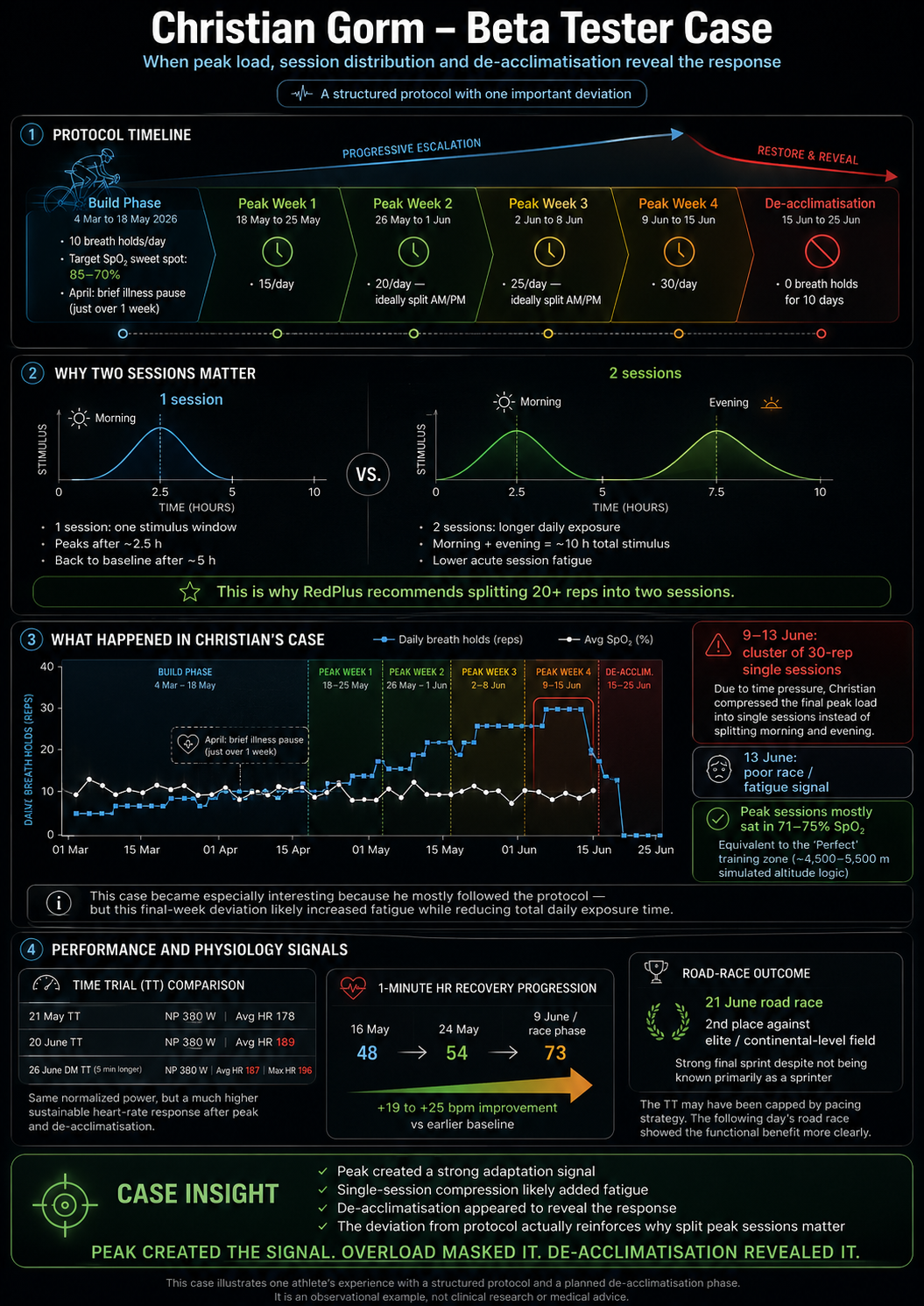
Christian Gorm, as a beta tester for RedPlus, has chosen to present his data from a longer structured breath-hold protocol. The case is interesting because Christian followed the RedPlus protocol very consistently for most of the period, but in the final part of the peak period he deviated from the protocol by completing 30 breath-holds in one session instead of distributing them across two daily sessions.
This deviation creates a particularly strong case angle because it both shows the value of the peak period and at the same time supports why RedPlus recommends correct distribution of high daily breath-hold volume. The case suggests that the peak period can create a powerful physiological stimulus, but that incorrect session distribution can increase acute fatigue and temporarily mask the positive adaptation.
After the de-acclimatisation period, Christian showed marked changes in heart-rate response, recovery and race performance.
1. Protocol progression
Christian started his RedPlus protocol on 4 March 2026. From 4 March to 18 May, he completed a longer build period with approximately 10 breath-holds per day.
He primarily stayed within RedPlus’ recommended hypoxic sweet spot, where SpO₂ typically lies around 85–70%. In April, Christian was affected by illness and had just over one week without breath-holds. After the illness period, he resumed the protocol and continued until the peak period. On 18 May, Christian started his four-week peak period:
• Peak week 1: 15 breath-holds/day
• Peak week 2: 20 breath-holds/day distributed across two sessions
• Peak week 3: 25 breath-holds/day distributed across two sessions
• Peak week 4: 30 breath-holds/day
In the final peak week, Christian had a busy schedule due to education, training and other commitments. Therefore, on several days he chose to complete all 30 breath-holds in one combined session instead of distributing them between morning and evening.
This is an important detail in the case.
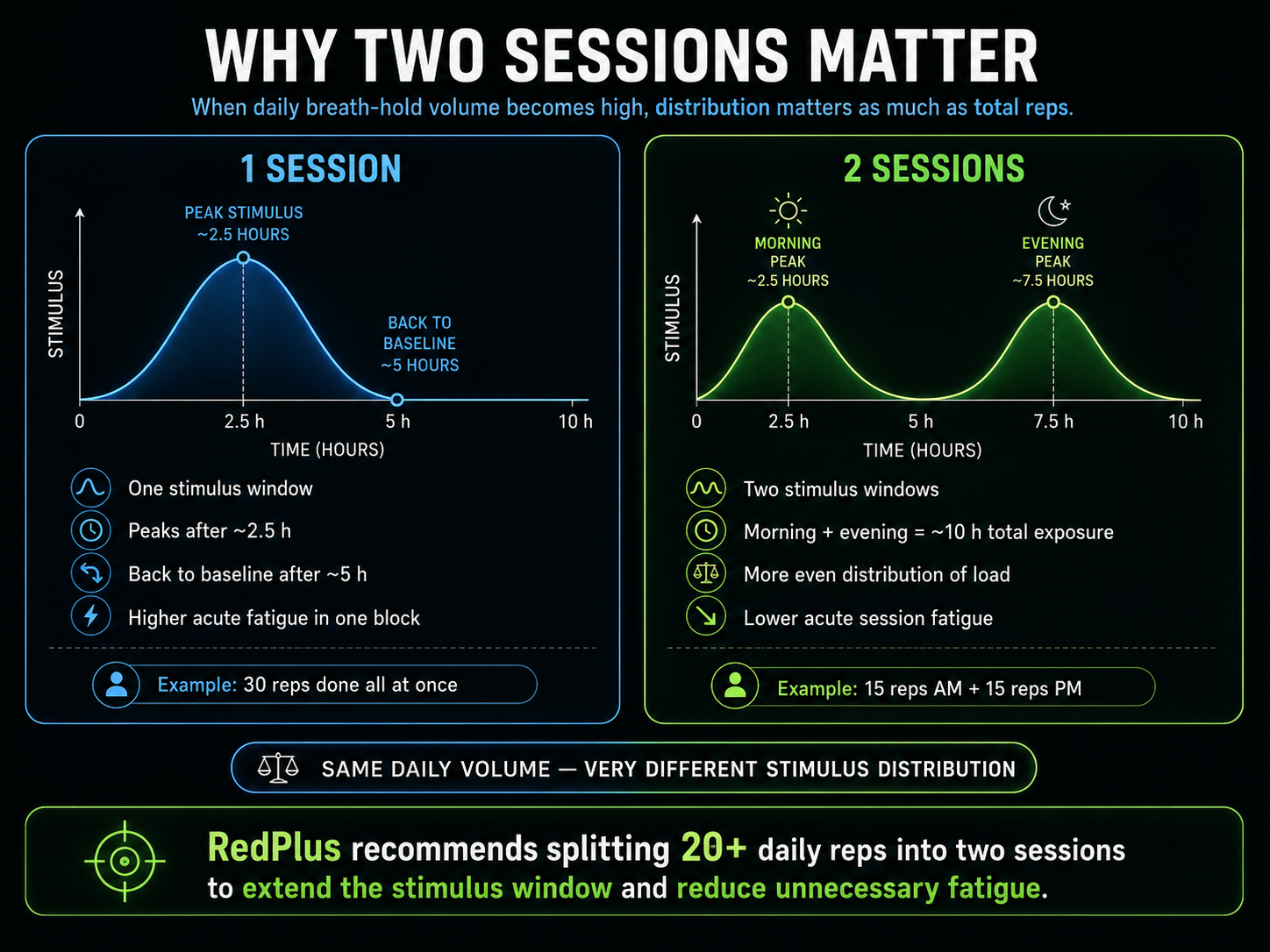
2. Why two sessions matter
RedPlus recommends that high daily breath-hold volume is distributed across two sessions when the volume reaches around 20–30 breath-holds/day.
The reason is that one single session is expected to create one stimulus window, where the response peaks after approximately 2.5 hours and gradually returns toward baseline after approximately 5 hours. If the entire daily volume is concentrated into one session, the athlete therefore receives a strong, but relatively short, stimulus window.
By distributing breath-holds across two sessions — for example morning and evening — two separate stimulus windows are created. This means that the athlete can be exposed to stimulus for up to approximately 10 hours in total instead of only approximately 5 hours. At the same time, the acute load per session is reduced.
The key point is therefore:
The same daily number of breath-holds can create very different physiological load depending on how they are distributed.
In Christian’s case, 30 breath-holds were collected into one session on several days. This may have created high acute fatigue without providing the same total stimulus distribution across the day as two sessions would have done.
3. The poor race on 13 June
On 13 June Christian raced in Denmark, where he did not feel good on the bike. At this point, he had just completed several days with 30 breath-holds in one combined session.
After the race, Christian had a conversation with RedPlus, where the assessment was that the concentrated peak load had most likely created too much acute fatigue. The interesting part is that this does not necessarily suggest that the peak period did not work. On the contrary, it may suggest that the peak load was powerful enough to create an adaptation, but that the acute fatigue temporarily masked the effect.
Christian was also made aware that he was now entering a 10-day de-acclimatisation period without breath-holds, and that there was a real possibility that he would experience a performance boost once the acute hypoxic load was removed.
This assessment later proved to be very interesting.
4. De-acclimatisation and performance boost
After completing the peak period, Christian entered the de-acclimatisation period. Here, he stopped doing breath-holds, but continued his normal training and race preparation.
Five days into the de-acclimatisation period, Christian rode a time trial in Denmark. Here, his data showed a markedly changed heart-rate response.
His previous 20-minute heart-rate record was normally around 178–180 beats/min. During the time trial after the peak period, his average heart rate was markedly higher, around 191 beats/min, and his heart-rate response showed that he could work at a higher cardiovascular level than before.
The important point is that his normalized power did not increase correspondingly. He still rode around 380 W normalized power, which was also the level in previous time trials. However, this does not necessarily mean that he did not have greater capacity. In a time trial, a rider typically rides according to a known pacing strategy. If Christian knew that he could normally hold around 380 W NP, it is natural that he tried to control the race around this level.
Therefore, the TT data should not be assessed on watts alone. The most interesting part is the change in physiological response at the same power.
5. Time trial data: same power, changed heart-rate response
Christian’s TT data show the following pattern:
• 21 May: approximately 380 W NP, average heart rate 178
• 20 June: approximately 380 W NP, average heart rate 189
• 26 June: Danish Championship TT: approximately 380 W NP, average heart rate 187, max heart rate 196
On 26 June, the time trial was also approximately five minutes longer, but Christian still held the same normalized power.
This means that at the same external output, he showed a markedly different cardiovascular response after the peak and de-acclimatisation period. He could work at a higher heart rate without reporting the same feeling of limitation, and he also showed improved recovery.
This points toward a changed physiological state, where the body may have had access to a larger cardiovascular reserve.
6. 1-minute HR recovery: a central signal
One of the strongest data points in Christian’s case is the change in his 1-minute heart-rate recovery.
His normal 1-minute recovery had previously been around 48–54 beats. During the peak period, this value increased markedly:
• 16 May: 48 bpm recovery
• 24 May: 54 bpm recovery
• 9 June: 73 bpm recovery
• after peak/de-load: around 73 bpm recovery
This is an improvement of approximately 19–25 beats compared with his previous baseline.
This is not a small change. It is a marked functional signal.
Faster heart-rate recovery can indicate improved autonomic regulation, faster parasympathetic reactivation and a better ability to recover after high-intensity load.
In cycling races, this is especially important because performance is not only about one maximal effort, but about the ability to repeatedly accelerate, respond to attacks, ride hard on climbs and then recover quickly again.
This fits precisely with Christian’s subsequent road race.
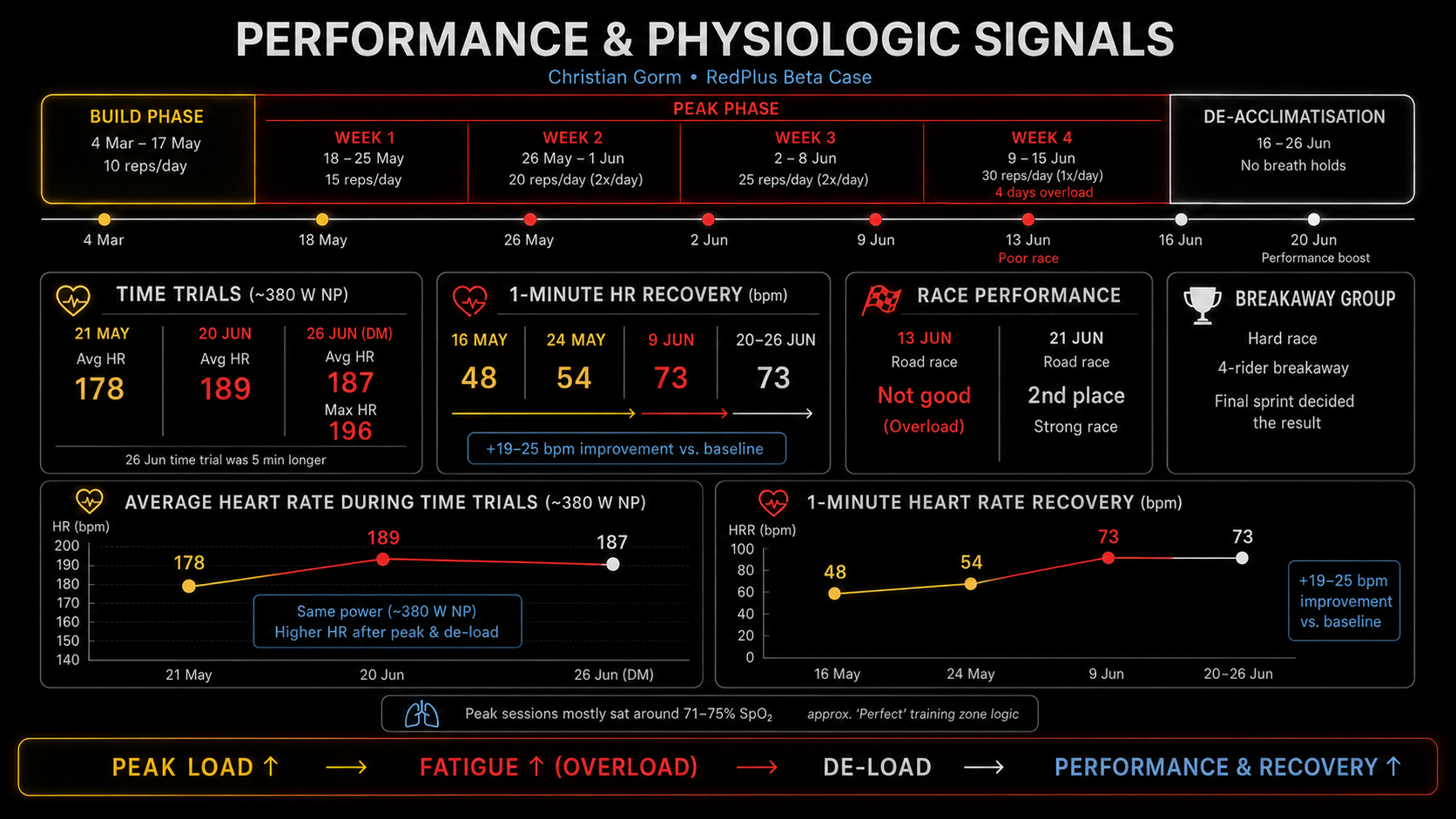
7. The road race: functional confirmation
The day after the time trial, Christian raced a road race in Denmark against a strong field consisting of elite, continental and some WorldTour-level riders.
Here, Christian finished second and, according to his own experience, was one of the strongest riders in the field. The race was decided from a smaller group, where four riders competed for the win. Christian lost by only a few centimeters in a breakaway group sprint.
This part of the case is important because a road race, more than a time trial, tests the ability to repeat hard efforts and recover quickly between loads. A time trial can be limited by pacing strategy. A road race forces the rider to respond to surges, climbs, attacks and tactical situations.
If Christian had improved recovery between hard efforts, a road race would be exactly the type of event where the effect could become more visible than in a controlled TT.
It is therefore relevant to view the road race as a functional confirmation of the physiological signals that could already be seen in the heart-rate and recovery data.
8. Possible explanation: peak created the signal, overload masked it, de-load revealed it
The overall case points toward a classic fitness-fatigue model.
The peak period may have created a powerful physiological stimulus. At the same time, the misplaced or incorrectly distributed final peak week may have created high acute fatigue. This can explain the poor race on 13 June.
When Christian then entered the de-acclimatisation period and stopped doing breath-holds, the acute hypoxic load dropped. If the adaptations from the build and peak period were still present, they could become more visible once the fatigue component decreased.
This fits with the subsequent development:
• poor performance immediately after heavy, compressed peak load
• markedly higher heart-rate response at the same TT power after de-load
• improved 1-minute HR recovery • strong road-race performance the following day
• continued strong TT performance at the Danish Championship
The short conclusion is:
Peak created the signal.
Overload masked it.
De-acclimatisation revealed it.
9. Possible blood-volume increase Several indicators in Christian’s case point toward a possible blood-volume increase, but the case lacks further evidence to conclude with certainty that blood volume actually increased.
The indicators pointing in that direction are:
• markedly changed heart-rate response after the peak and de-acclimatisation period
• improved 1-minute HR recovery
• the ability to work at a higher heart rate without a corresponding negative experience
• strong performance in a hard road race the day after the TT
• the same type of response pattern as observed in other RedPlus cases
• a protocol that can theoretically create haematological and cardiovascular adaptation
An increase in total blood volume could potentially explain several of the observations. Increased total blood volume can improve venous return, increase cardiac filling, support greater stroke volume and thereby increase overall cardiovascular capacity. If red-cell volume or total haemoglobin mass also increased, this could further improve oxygen transport.
It is important to emphasise that Christian’s case does not in itself document a blood-volume increase. To conclude this with high certainty, further testing is required, for example blood tests before and after the peak period, and ideally measurements of total haemoglobin mass, plasma volume and total blood volume.
The correct conclusion is therefore:
Several indicators in Christian’s case are consistent with a possible increase in total blood volume, and the pattern resembles observations from other RedPlus cases. However, the mechanism requires further testing before it can be confirmed with certainty.
10. Why the case is important for RedPlus
The Christian Gorm case is important for three reasons.
First, it shows that a structured build and peak period can be associated with marked changes in heart-rate response, recovery and race performance.
Second, it shows that session distribution is critical. The case supports RedPlus’ recommendation to distribute high daily breath-hold volume across two sessions. When 30 breath-holds are collected into one session, fatigue can increase without the stimulus window necessarily being extended optimally.
Third, the case shows the value of de-acclimatisation. The 10-day period without breath holds appears to have removed acute load and made it possible for Christian to express the adaptation built during the build and peak period.
This makes the case particularly interesting, because the deviation from the protocol actually strengthens the understanding of the protocol. If Christian had followed the protocol perfectly, the case would probably still have been interesting. But because he deviated from it in the most demanding part of the peak period, the data show more clearly why correct dosing and timing matter.
11. Preliminary conclusion
Christian Gorm’s data show a clear response pattern after a structured RedPlus protocol:
• long build period • progressive peak period
• compressed overload in the final peak week
• poor performance shortly after overload
• subsequent de-acclimatisation
• markedly changed heart-rate response
• improved 1-minute HR recovery
• strong road-race performance
• continued strong TT performance
The case suggests that the RedPlus protocol can create a measurable physiological and performance-related response, especially when the peak period is followed by correct de acclimatisation.
Several indicators point toward a possible blood-volume increase, but this requires further testing before it can be confirmed with certainty. The case should therefore be understood as a strong performance and physiology case, not as final proof of one specific mechanism.
The most important learning is:
When peak load becomes high, distribution is decisive. When acute fatigue is removed, adaptation can become visible. And in Christian’s case, several independent signals point in the same direction: improved cardiovascular response, faster recovery and stronger functional performance.